Home » Acupuncture
Category Archives: Acupuncture
Substitution of Acupuncture for HCG in Ovulation Induction
Cai Xuefen
Obstetrical & Gynecological Hospital,
Zhejiang Medical University, Zhejiang Province 310006
Source: Journal of Traditional Chinese Medicine 17 (2):119-121,1997
By using human menopausal gonadotropin (HMG) and human chorionic gonadotropin (HCG), fairly good clinical therapeutic efficacy has been obtained in the treatment of infertility. However, difficulties are brought about due to the ovarian hyperstimulation syndrome (OHSS) easily induced by these two drugs. Therefore, we attempted to use acupuncture instead of HCG in the induction of ovulation from 1989 to 1992, and satisfactory therapeutic effect was achieved as reported in the following.
General Data
Ten patients were hospitalized with confirmed diagnosis of infertility and totally observed for 11 menstrual cycles (one patient had recurrence of OHSS for 2 times). Their ages ranged from 27 to 30 years with an average of 29 years. After treatment by HMG, all patients manifested OHSS in varying degrees. In accordance with the criteria for grading of OHSS issued by WHO, among these 11 menstrual cycles 4 cycles were mild (ovarian slight enlargement less than 5 cm with symptoms of slight malaise of lower abdomen); 7 were moderate (marked enlargement of ovary with nausea, vomiting and abdominal distension); no severe case occurred (extreme enlargement of ovary with hydrothorax, ascites, pycnemia and electrolyte disturbance). In order to prevent the exacerbation of OHSS caused by combined use of HMG and HCG, acupuncture was used after HMG treatment to replace HCG for the ovulation induction in 11 menstrual cycles of these patients.
Therapeutic Method
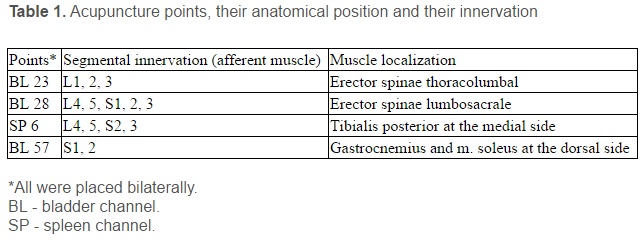
1.5-3 cun long filiform needles (no. 28-30) were used. The acupoints used for needling were Zigong (Extra 16), Shenshu (UB 23), Ciliao (UB 32), (the above acupoints were used bilaterally) and Guanyuan (Ren 4). Baohuang (UB 53) and Zhongji (Ren 3) were selected according to the signs and symptoms as adjuvant points. The manipulation techniques included twirling, rotating, lifting and thrusting. Reinforcing method was used in Shenshu point and the remaining points were punctured by reducing manipulation. The needling sensation should be transmitted toward both sides of lower abdomen. When arrival of Qi, retained the needles for 15 min. and manipulated the needles intermittently during the retaining period to enhance the stimulation. Moxibustion with moxa stick was used for some of these acupoints.
Observation of Therapeutic Effect
Criteria for assessment of therapeutic effect: Therapeutic effect was appraised mainly by comparison of ultrasonic B examination after needling with that before treatment and referred to the score of cervix uteri and basal body temperature to sit judgment on ovulation. Ovulation occurred within 24 h after 1st needling was considered as marked effect; ovulation within 72 h after 2-3 times of needling was effective; no ovulation occurred after 72 h after more than 3 times of needling was scored as ineffective.
Results of Treatment
Of the 11 menstrual cycles, marked effect was shown in 5 cycles, effective in 5 cycles and failed in 1 cycle. Among the 10 markedly effective and effective cycles, ovulation was induced in 2 cases after needling and diagnosed pregnancy by blood HCG assay and ultrasonography. In 9 of the 10 cycles treated with acupuncture for ovulation induction without using HCG and other drugs, the symptoms of OHSS were significantly remitted or even disappeared. Only in one cycle, HCG (with dosage less than for ovulation) was used after needling to maintain the function of corpus luteum and resulted in exacerbation of OHSS and finally remitted by drug treatment.
Typical Case
Fang, 27-year-old, suffered from polycystic ovary syndrome. She was unpregnant after married 2 years and the menstruation was only 1-2 times a year. The basal body temperature was monophase. No effect was observed using clomiphene and then treated with HMG. From the day 5, for bleeding due to withdrawal of progesterone, intramuscular injection of HMG was given at a dose of 150 U once a day for 8 days. The score of cervix uteri was 12 mark. The ultrasonogram showed that the size of right ovary was 9.6 cm x 7.8 cm x 4.6 cm and the left side was 9.2 cm x 7.2 cm x 4.7 cm. Both sides of ovary had 10-20 follicles with maximum size 1.8 cm. In order to avoid severe OHSS, acupuncture was used instead of HCG for ovulation induction after stopping HMG treatment. On the next day after the first needling, the basal body temperature elevated from 36.3°C to 36.8°C and the score of cervix uteri fell from 12 mark to 9 mark, and ultrasonic B examination suggested that part of the follicles were ovulated. After the l9th day of ovulation, the blood concentration of HCG started rising and after 40 days the blood level of HCG reached to 35.6 ng/ml. The ultrasonogram showed that the diameter of embryonic sac was 1.5 cm and early pregnancy was diagnosed.
Discussion
It was reported in literature that using HMG-HCG in the induction of ovulation, the ovulatory rate was about 70%-90%, but the incidence of OHSS might be 10%-15.4% and even life-threatening in the severe case. At present, there were no satisfactory measures for the prevention and remission of OHSS. In most reports, it is considered that when OHSS inclines to occur, stopping injection of HCG is the effective way to avoid severe OHSS. However, stopping HCG would not only discontinue the ovulation of HCH, but also gave up the already developed follicles. Our clinical practice demonstrated that acupuncture is effective in ovulation induction and also the remission of OHSS induced by HMG. Furthermore, we also noted that in most OHSS patients enlarged ovaries and numerous developed follicles were revealed. As a result of excessive follicles developed, dysplasia of ova and insufficiency of corpus luteum often occurred, thus leading to uneasy pregnancy after ovulation. So it is reasonable to infer that using some Chinese drugs benefiting the function of corpus luteum or using certain amount of progesterone as supplementary treatment after acupuncture, the pregnancy rate could be raised.
A Brief Introduction to the Training Center of China Academy of Traditional Chinese Medicine
The Training Center of China Academy of Traditional Chinese Medicine is an educational institution of traditional Chinese medicine, and has excellent teachers and good bases for clinical practice and provides proper board and lodging.
The Center regularly conducts three-month advanced and general courses of traditional Chinese medicine, acupuncture, Tuina (massage), Qigong (breathing exercises) and Taiji (shadow boxing). It also runs short-term training courses on some special topics, and preparatory guidance courses for licensure examination of tradi tional Chinese medicine, acupuncture and moxibustion. In addition, various courses based on the participant’s requirements may be arranged in the center. All those who complete the required courses will receive relevant certificates.
The Training Center is always ready to establish friendly relations of exchange and cooperation with medical institutions of various countries. It warmly welcomes medical professionals from home and abroad to take training courses.
Address: Training Center of China Academy of Traditional Chinese Medicine
No 18 Beixincang Dongzhimennei, Beijing 100700 China
Dr. Pan Ping Dr. Zhao Jihui
Tel: 86-10-64075193 64062096
Fax: 86-10-64061635 64062096
Role of acupuncture in the treatment of female infertility
Raymond Chang, M.D.[a,b] Pak H. Chung, M.D.[b] and Zev Rosenwaks, M.D.[c]
The Institute of East-West Medicine and the Center for Reproductive Medicine and Infertility, Weill Medical College of Cornell University, New York, New York
Received June 24, 2002; revised and accepted July 19, 2002.
Reprint requests: Pak H. Chung, M.D., The Center for Reproductive Medicine and Infertility, Weill Medical College of Cornell University, 505 East 70 Street, New York, New York 10021 (FAX: 212-746-8208; E-mail: pakchu@med.cornell.edu).
[a]The Institute of East-West Medicine. [b]The Department of Internal Medicine, Weill Medical College of Cornell Unversity. [c]The Center for Reproductive Medicine and Infertility. 0015-0282/02/$22.00 PII S0015-0282(02)04348-0
Objective: To review existing scientific rationale and clinical data in the utilization of acupuncture in the treatment of female infertility.
Design: A MEDLINE computer search was performed to identify relevant articles.
Result(s): Although the understanding of acupuncture is based on ancient medical theory, studies have suggested that certain effects of acupuncture are mediated through endogenous opioid peptides in the central nervous system, particularly ß-endorphin. Because these neuropeptides influence gonadotropin secretion through their action on GnRH, it is logical to hypothesize that acupuncture may impact on the menstrual cycle through these neuropeptides. Although studies of adequate design, sample size, and appropriate control on the use of acupuncture on ovulation induction are lacking, there is only one prospective randomized controlled study examining the efficacy of acupuncture in patients undergoing IVF. Besides its central effect, the sympathoinhibitory effects of acupuncture may impact on uterine blood flow.
Conclusion(s): Although the definitive role of acupuncture in the treatment of female infertility is yet to be established, its potential impact centrally on the hypothalamic-pituitary-ovarian axis and peripherally on the uterus needs to be systemically examined. Prospective randomized controlled studies are needed to evaluate the efficacy of acupuncture in the female fertility treatment. (Fertil Steril® 2002;78:1149-53. ©2002 by American Society for Reproductive Medicine.
Key Words: Acupuncture, female infertility, in vitro fertilization
Acupuncture as a therapeutic intervention has been extensively studied and is increasingly practiced in the United States. A recent survey of acupuncture released by an NIH Consensus Development panel (1) indicated that although there are inherent problems of design, sample size, and appropriate controls in the acupuncture literature, promising data exist for the use of acupuncture in treating nausea and vomiting (2), postoperative pain (3-5), addiction (6-9), and general pain syndromes (10-12). As a medical technique, acupuncture has also been reported as an adjunct in the treatment of various gynecologic problems (13-15).
Although conventional treatment options for female infertility have been well established, there have been few systematic reviews of complementary or alternative approaches to the treatment of infertility. In light of an increasing trend in the use of complementary and alternative medicine (16) and common inquiry and utilization of such approaches by patients suffering from infertility, we intend to review the existing scientific rationale and clinical data based on which acupuncture may exert an influence on the outcome of female fertility.
In examining the potential usefulness of acupuncture in enhancing female fertility, it is appropriate first to give some theoretical background for acupuncture. Although the theory of acupuncture stems from underlying traditional Chinese medicine premises that would define etiologies for infertility in terms of energy disturbance of imbalances, or organ deficiencies and excesses, we intend to review the existing literature by examining modern medical aspects of the central and peripheral modes of action of acupuncture as they impact on the hypothalamic-pituitary-ovarian axis and the pelvic organs, respectively. Moreover, the effect of acupuncture on anxiety and stress and ensuing potential indirect effects on female fertility will also be discussed.
Background
Acupuncture is the manipulation of thin metallic needles inserted into anatomically defined locations on the body to affect bodily function. The US Food and Drug Administration has recently removed acupuncture needles from the category of experimental medical devices and now regulates them just like it does other devices, such as surgical scalpels and hypodermic needles, under good manufacturing practices and single-use standard of sterility (1).
The general theory of acupuncture is based on the premise that there are patterns of energy flow (Qi) through the body, which are essential for health. Disruption of this flow is believed to be responsible for disease. Acupuncture can correct imbalances of flow at identifiable points close to the skin.
According to the proposed international acupuncture nomenclature by The World Health Organization in 1991 (17), the meridian system consists of 20 meridians interconnecting about 400 acupoints. These acupoints correspond to specific areas on the surface of the body, which demonstrate higher electrical conductance because of the presence of higher density of gap junctions along cell borders. They act as converging points (or sinks) for electromagnetic fields. A higher metabolic rate, temperature, and calcium ion concentration, are also observed at these points. In principle, positive (anode) pulse stimulation of a point inhibits the organ function, whereas negative (cathode) pulse stimulation enhances that function (18). This forms the basis of electroacupuncture, which applies small electrical needles inserted in specific acupoints.
Effects of acupuncture on the hypothalamic-pituitary-ovarian axis and menstrual cycle
Although traditional Chinese medicine understanding of acupuncture is based on ancient medical theory, a modern and scientific neuroendocrine perspective has begun to evolve in the past two decades. Mayer et al. (19) first reported that acupuncture analgesia was induced through endorphin production and antagonized by the narcotic antagonist naloxone. Other studies similarly suggested that certain effects of acupuncture are mediated through the nervous system, within which ß-endorphin and other neuropeptides have been implicated (20-22).
Acupuncture was shown by Petti et al. (20) to cause a significant increase in ß-endorphin levels during treatment, which lasted for up to 24 hours. ß-endorphin is derived from its precursor protein pro-opiomelanocortin, which is present in abundant amounts in neuronal cells of the arcuate nucleus of the hypothalamus, pituitary, medulla, and in peripheral tissues including intestines and ovaries (23-25). Pro-opiomelanocortin cleaves to form adrenocorticotropic hormone and ß-lipoprotein. Further cleavage of ß-lipoprotein yields neuropeptides including ß-endorphin. Aleem et al. (26, 27) demonstrated the presence of immunoreactive ß-endorphin in follicular fluids of both normal and polycystic ovaries.
The influence on gonadotropin secretion and the menstrual cycle by endogenous opioid peptides is believed to be mediated by their action on GnRH secretion (28). The hypothalamic ß-endorphin center and the GnRH pulse generator, in fact, are both situated within the arcuate nucleus. Quigley et al. (29) first reported an increased opioid inhibition of LH secretion in hyperprolactinemic patients with pituitary microadenomas. Ching (30) and Orstead and Spics (31), respectively, showed that opioid peptides suppress GnRH release in rats and rabbits.
The role of these neuropeptides, including ß-endorphin, in the regulation of GnRH secretion in humans has recently been reviewed by Kalra et al. (32) and Pau and Spies (33). Rossmanith et al. (34) demonstrated the role of opioid peptides in the initiation of the mid-cycle LH surge in normal cycling women. Meanwhile, measurement of ß-endorphin in ovarian follicular fluid of healthy ovulatory women revealed much higher levels than that in circulating plasma (35). The highest level of ß-endorphin was noted to be in the preovulatory follicle.
Because acupuncture treatment impacts on ß-endorphin levels, which in turn affect GnRH secretion and the menstrual cycle, it is logical to hypothesize that acupuncture may influence ovulation and fertility. Animal studies have revealed that acupuncture treatment normalized GnRH secretion and affected peripheral gonadotropin levels (36, 37). Various investigators have shown that in normally ovulatory or anovulatory women, acupuncture also influenced plasma levels of FSH, LH, E2, and P (38-40). Acupuncture as a surrogate for hCG in ovulation induction was successfully used by Cai (41). Chen and Yu (42) showed that electroacupuncture normalized they hypothalamic-pituitary-ovarian axis, and in another study Chen (43) reported that 6 of 13 anovulatory cycles responded to acupuncture treatment.
A series published from the University of Heidelberg in Germany (44) used auricular acupuncture on 45 infertile women suffering from ovulatory dysfunction such as oligomenorrhea and luteal phase defect. The control group received medical treatment including bromocriptine, dexamethasone, levothyroxine, clomiphene citrate (CC), and gonadotropin. Although the investigators concluded that resumption of ovulatory cycles occurred significantly more often in the acupuncture group compared to the control group, pregnancy rates were not different between the two groups. However, interpretation of study data was very difficult due to the heterogeneity of the patient population and treatment modalities. Moreover, seven pregnancies in the acupuncture group were actually achieved with hormone treatment 6 months after acupuncture was stopped.
Another study by Stenver-Victorin et al. (45) evaluated the use of electroacupuncture for ovulation induction on 24 oligo/amenorrheic women with polycycstic ovarian syndrome (PCOS). The percentage of ovulatory cycles in all subjects was shown to improve from 15% (in a total of 3 months before treatment) to 66% up to 3 months after treatment. Responsive patients were noted to have significantly lower body mass index (BMI), waist-to-hip circumference ratio, serum T concentration, serum T/sex hormone-binding globulin ratio, and serum basal insulin level. They suggested that, in these selected patients with PCOS, acupuncture could be considered as an alternative or adjunct to pharmacological ovulation induction.
A recent prospective randomized controlled study by Paulus et al. (46) compared pregnancy rates in a total of 160 patients undergoing IVG. Acupuncture was performed in 80 patients 25 minutes before and after ET. After controlling confounding variables, clinical pregnancy rate for the acupuncture group (42.5%) was significantly higher than the control group (26.3%).
Peripheral effects of acupuncture
In addition to the central modulation of the hypothalamic-pituitary-ovarian axis, the effects of acupuncture on the autonomic nervous system have been well documented (47). In the early 1980s, Yao et al. (48) reported long-lasting cardiovascular depression induced by acupuncture stimulation of the sciatic nerve in unanesthetized hypertensive rats. In the human, acupuncture was also shown to be sympathoinhibitory. After acupuncture, sympathetic nerve activity as measured by norepinephrine level, skin temperature, blood pressure, and pain tolerance threshold was shown to be decreased (49).
Endometrial thickness, morphology, and uterine artery blood flow have been implicated as important parameters for success of implantation of human embryos (50-57). Despite conflicting results in the utilization of these parameters during various stages of treatment to predict outcome in IVF, it is generally believed that adequate endometrial thickness is required to optimize pregnancy rate. Because endometrial thickness is a function of uterine artery blood flow, Sher and Fisch (58) reported a novel method of using vaginal sildenafil in an attempt to improve uterine artery blood flow and endometrial development in patients undergoing IVF.
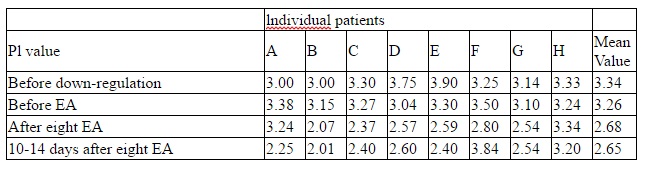
With its central sympathoinhibitory effect, acupuncture may contribute to reduce uterine artery impedance and therefore, increase blood flow to the uterus. In fact, Sterner-Victorin et al. (59) demonstrated this when they performed acupuncture in 10 infertile women who were down-regulated by GnRH analog to avoid the effect of endogenous hormone on the uterine artery blood flow.
Pulsatility index in the uterine artery and skin temperature (on the forehead and lumbosacral area) were evaluated in three time periods-before, right after, and 2 weeks after acupuncture treatment (twice a week for 4 weeks). Pulsatility index and skin temperatures were found to be significantly decreased and increased, respectively, both right after and 14 days after acupuncture treatment. This effect was hypothesized to be caused by central inhibition of sympathetic activity.
Acupuncture and stress reduction
It has been well documented that infertility causes stress (60-65), and stress reduction may, in turn, improve fertility (66). However, the relationship between stress and infertility is that of a vicious cycle. Social stigmatization, decreased self-esteem, unmet reproductive potential of sexual relationship, physical and mental burden of treatment, and the lack of control on treatment outcome are just some of the factors that can lead to psychological stress in any couple pursuing infertility treatment. In turn, stress may lead to the release of stress hormones and influence mechanisms responsible for a normal ovulatory menstrual cycle through its impact on the hypothalamic-pituitary-ovarian axis.
The use of acupuncture for reducing anxiety and stress possibly through its sympathoinhibitory property and impact on ß-endorphin levels has been reviewed (67, 68), and the efficacy of acupuncture in depression has also been studied (69). Because the pharmacological side effects of anxiolytic and antidepressant drugs on infertility treatment outcome are largely unknown, acupuncture may provide an excellent alternative for stress reduction in women undergoing infertility treatment.
Discussion
The practice of acupuncture to treat identifiable patho-physiological conditions has been a subject of intense research. The underlying physiologic mechanisms of acupuncture such as the release of opioids and other peptides in the central peripheral nervous system, and its inhibition of the sympathetic nervous system have been increasingly established. Promising results from credible trials have emerged for the use of acupuncture in treating various pain syndromes, substance abuse, and chemotherapy-induced nausea and vomiting.
Although the definitive role of acupuncture in the treatment of female infertility is yet to be established, its neuroendocrine effect on the hypothalamic-pituitary-ovarian axis and the preliminary clinical data reviewed here justifies further clinical trials to systematically examine the efficacy of acupuncture in treating various conditions related to female infertility such as ovulatory dysfunction associated with PCOS. The peripheral impact of acupuncture in improving uterine artery blood flow and hence endometrial thickness also provides encouraging data regarding its potential positive effect on implantation.
Whether these potential beneficial effects of acupuncture on the reproductive system can be translated into improving infertility treatment outcomes will eventually mandate randomized controlled studies of adequate design. Because acupuncture is nontoxic and relatively affordable, its indications as an adjunct in assisted reproduction or as an alternative for women who are intolerant, ineligible, or contraindicated for conventional hormone induction of ovulation deserves serious research and exploration.
Appropriate training, credentialing, and certification of acupuncture practitioners by state agencies can facilitate the integration of acupuncture into the treatment of female infertility, and healthcare in general. The NIH Consensus Conference (1) agreed that this is necessary to allow the public and other health practitioners to identify qualified acupuncture practitioners. With the help of the US Department of Education, issues of training and licensure of non-physician and physician practitioners have been addressed. There is sufficient evidence to acupuncture’s value to expand its use into conventional medicine and treatment of female infertility, and to encourage further studies of its underlying mechanisms as well as to establish its clinical value.
References
1. NIH Consensus Development Panel of Acupuncture. Acupuncture. JAMA 1998;280:1518-24.
2. Dundee JW, Ghaly RG, Lynch GA, Fitzpatrick KT, Abram WP. Acupuncture prophylaxis of cancer chemotherapy-induced sickness. J R Soc Med 1989;82:268-71.
3. Christiansen PA, Noreng M, Andersen PE, Nielsen JW. Electroacupuncture and postoperative pain. Br J Anaesth 1989;62:258-62.
4. Martelete M, Fiori AMC. Comparative study of analgesic effect of transcutaneous nerve stimulation (TNS), electroacupuncture (EA), and meperidine in the treatment of postoperative pain. Acupunct Electrother Res 1985;10:183-93.
5. Lao L, Bergman S, Langenberg P, Wong RH, Berman B. Efficacy of Chinese acupuncture on postoperative oral surgery pain. Oral Surg Med Oral Path Oral Radiol Endod 1995;79:423-8.
6. Bullock ML, Culliton PD, Olander RT. Controlled trial of acupuncture for severe recidivist alcoholism. Lancet 1989;1:1435-39.
7. Clavel-Chapelon F, Paoletti C, Banhamou S. Smoking cessation rates 4 years after treatment by nicotine gum and acupuncture. Prev Med 1997;26:25-8.
8. He D, Berg JE, Hostmark AT. Effects of acupuncture on smoking cessation or reduction for motivated smokers. Pev Med 1997;26:208-14.
9. Margolin A, Avants SK, Chang P, Kosten TR. Acupuncture for the treatment of cocaine dependence in methadone-maintained patients, Am J Addict 1993;2:194-201.
10. Patel M, Gutzwiller F, Paccaud F, Marazzi A. A meta-analysis of acupuncture for chronic pain. Int J Epidemiol 1989;18:900-6.
11. Shlay JC, Chaloner K, Max MB, Flaws B, Reichelderfer P, Wentworth D, et al. Acupuncture and amitriptyline for pain due to HIV-related peripheral neuropathy: a randomized control trial. JAMA 1998;280:1590-5.
12. Tier Riet G, Kleijnen J, Knipschild P. Acupuncture and chronic pain: a criteria based meta-analysis. J Clin Epidemiol 1990;43:1191-9.
13. Chez RA, Jonas WB. Complementary and alternative medicine. Part II: Clinical studies in gynecology. Obstet Gynecol Surv 1997;52:709-16.
14. Wu XJ, Cui YL, Yang BY, Zhou QM, Observations on the effect of He-Ne laser acupoint radiation in chronic pelvic inflammation. J Tradit Chin Med 1987;7:263-5.
15. Beal MW. Acupuncture and acupressure. Applications to women’s reproductive health care. J Nurse Midwifery 1999;44:217-30.
16. Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA 1998;280:1569-75.
17. World Health Organization. A proposed standard international acupuncture nomenclature: report of a WHO scientific group. Geneva, Switzerland: World Health Organization, 1991.
18. McCaig CD. Sinal neurite reabsorption and regrowth in vitro depend on the polarity of an applied electric field. Development 1987;100:31-41.
19. Mayer DJ, Price DD, Rafil A. Antagonism of acupuncture analgesia in man by the narcotic antagonist naloxone. Brain Res 1977;121:368-72.
20. Petti F, Bangrazi A, Liguori A, Reale G, Ippoliti F. Effects of acupuncture on immune response related to opioids-like peptides. J Tradit Chin Med 1998;18:55-63.
21. Ulett GA, Han S, Han JS. Electroacupuncture: mechanisms and clinical application, Biol Psychiatry 1998;44:129-38.
22. Ku Y, Chang Y. Beta-endorphin and GABA-mediated depressor effect of specific electroacupuncture surpasses pressor response of emotional circuit. Peptides 2001;22:1465-70.
23. Facchinetti F, Storchi AR, Petraglia F, Volpe A, Genazzani AR. Expression of proopiomelanocortin-related eptides in human follicular fluid. Peptides 1988;9:1089-92.
24. Gallinelli A, Garuti G, Matteo ML, Genazzani AR, Facchinetti F. Expression of proopiomelanocortin gene in human ovarian tissue. Hum Reprod 1995;10:1085-9.
25. DeBold CD, Menefee JK, Nicholson WE, Orth DN. Proopiomelanocortin gene is expressed in many normal human tissues and intumors not associated with ectopic adrenocorticotropin syndrome. Mol Endocrinol 1988;2:862-70.
26. Aleem FA, Eltabbakh GH, Omar RA, Couthren AL. Ovarian follicular fluid beta-endorphin levels in normal and polycystic ovaries. Am J Obstet Gynecol 1987;156:1197-200.
27. Aleem FA, Omar RA, Eltabbakh GH. Immunoreative beta-endorphin in human ovaries. Fertial Steril 1986;45:507-11.
28. Ferin M, Van de Wiele RL. Endogenous opioid peptides and the control of the menstrual cycle. Eur J Obstet Gynecol Repro Biol 1984;10:365-73.
29. Quigley ME, Sheeham KL, Casper RF, Yen SSC. Evidence for an increased opioid inhibition of luteinizing hormone secretion in hyperprolactinemic patients with pituitary microadenoma. J Clin Endocrinol Metabol 1980;50:427-46.
30. Ching M. Morphine suppresses the proestrous surge of GnRH in pituitary portal plasma of rats. Endocrinology 1983;112:2209-11.
31. Orstead KM, Spics HG. Inhibition of hypothalamic gonadotropin releasing hormone release by endogenous opioid peptides in the female rabbit. Neuroendocrinology 1987;46:14-23.
32. Kalra SP, Horvath T, Naftolin F, Xu B, Pu S, Kalra PS. The interactive language of the hypothalamus for the gonadotropin releasing hormone (GNRH) system. J Neuroendocrinol 1997;9:569-76.
33. Pau KY, Spies HG. Neuroendocrine signals in the regulation of gonadotropin-releasing hormone secretion. Chin J Physiol 1997;40:181-96.
34. Rossmanith WG, Mortola JF, Yen SSC. Role of endogenous opioid peptides in the initiation of the mid-cycle luteinizing hormone surge in normal cycling women. J Clin Endocrinol Metab 1988;67:695-700.
35. Petraglia F, DiMeo G, Storchi R, Segre A, Facchinette F, Szalay S, et al. Proopiomelanocortin-related peptides and methionine enkephalin in human follicular fluid: changes during the menstrual cycle. Am J Obstet Gynecol 1987;157:142-6.
36. Lin JH, Liu SH, Chan WW, Wu LS, Pi WP. Effects of electroacupuncture and gonadotropin-releasing hormone treatments on hormone changes in anoestrous sows. Am J Chin Med 1988;16:117-26.
37. Yang SP, Yu J, He L. Release of gonadotropin-releasing hormone (GnRH) from the medio-basal hypothalamus induced by electroacupuncture in conscious female rabbits. Acupunct Electrother Res 1994;19:19-27.
38. Aso T, Motohashi T, Murata M, Nishimura T, Kakizaki K. The influence of acupuncture stimulation on plasma levels of LH, FSH, progesterone and estradiol in normally ovulating women. Am J Chin Med 1976;4:391-401.
39. Yu J, Zheng HM, Ping SM. Changes in serum FSH, LH and ovarian follicular growth during electroacupuncture for induction of ovulation [Chinese]. Chung His I Chieh Ho Tsa Chih 1989;9:199-202.
40. Mo X, Li D, Pu Y, Xi G, Le X, Fu Z. Clinical studies on the mechanism of acupuncture stimulation of ovulation. J Trad Chin Med 1993;13:115-9.
41. Cai X. Substitution of acupuncture for human chorionic gonadortropin in ovulation induction. J Tradit Chin Med 1997;17:119-21.
42. Chen BY, Yu J. Relationship between blood radioimmunoreactive beta-endorphin and hand skin temperature during the electro-acupuncture induction of ovulation. Acupunct Electrother Res 1991;16:1-5.
43. Chen BY. Acupuncture normalizes dysfunction of hypothalamic-pituitary-ovarian axis. Acupunct Electrother Res 1997;22:97-108.
44. Gerhard I, Postneek F. Auricular acupuncture in the treatment of female infertility. Gynecol Endocrinol 1992;6:171-81.
45. Stener-Victorin E. Waldenstrom U, Tagnfors U, Lundeberg T, Lundstedt G, Janson PO. Effects of electro-acupuncture on anovulation in women with polycycstic ovary syndrome. Acta Obstet Gynecol Scand 2000;79:180-8.
46. Paulus WE, Zhang M, Strehler E, El-Danasouri I, Sterzik K. Influence of acupuncture on the pregnancy rate inn patients who undergo assisted reproduction therapy. Fert Steril 2002;77:721-4.
47. Haker E, Egekvist H, Bjerring P. Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. J Automomic Nerv Sys 2000;79:52-9.
48. Yao T, Andersson S, Thoren P. Long-lasting cardiovascular depression induced by acupuncture-like stimulation of the sciatic nerve in unanaesthetized spontaneously hypertensive rats. Brain Res 1982;240:77-85.
49. Knardahl S, Elam M, Olausson B, Wallin BG. Sympathetic nerve activity after acupuncture in humans. Pain 1998;75:19-25.
50. Noyes N, Liu HC, Sultan K, Schattman G, Rosenwaks Z. Endometrial thickness appears to be a significant factor in embryo implantation in thickness appears to be a significant factor in embryo implantation in-vitro fertilization. Hum Reprod 1995;10:919-22.
51. Schild RL, Knoblock C, Dorn C, Fimmers R, van der Ven H, Hansmann M. Endometrial receptivity in an in vitro fertilization program as assessed by spiral artery blood flow, endometrial thickness, endometrial volume, and uterine artery blood flow. Fertil Steril 2001;75:361-6.
52. Chiang CH, Hsieh TT, Chang MY, Shiau CS, Hou HC, Hsu JJ, et al. Prediction of pregnancy rate of in vitro fertilization an embryo transfer in women aged 40 and over with basal uterine artery pulsatility index. J Assist Reprod Genet 2000;17:409-14.
53. Engmann L. Sladkevicius P, Agrawal R, Bekir J, Campbell S, Tan SL. The pattern of changes in ovarian stromal and uterine artery blood flow velocities during in vitro fertilization treatment and its relationship with outcome of the cycle. Ultrasound Obstet Gynecol 1999;13:26-33.
54. Salle B, Bied-Damon V, Benchaib M, Desperes S, Gaucherand P, Rudigoz RC. Preliminary report of an ultrasonography and colour Doppler uterine score to predict uterine receptivity in an in-vitro fertilization programme. Hum Reprod 1998;13:1669-73.
55. Aytoz A, Ubaldi F, Tournaye H, Nagy ZP, Van Steirteghem A, Devroey P. The predictive value of uterine artery blood flow measurements for uterine receptivity in an intracytoplasmic sperm injection program. Fertil Steril 1997;68:935-7.
56. Friedler S, Schenker JG, Herman A, Lewin A. The role of ultrasonography in the evaluation of endometrial receptivity following assisted reproductive treatments: a critical review. Hum Reprod Update 1996; 2:323-35.
57. Zaidi J, Pittrof R, Shaker A, Kyei-Mensah A, Campbell S, Tan SL. Assessment of uterine artery blood flow on the day of human chorionic gonadotropin administration by transvaginal color Doppler ultrasound in an in vitro fertilization program. Fertil Steril 1996;65:377-81.
58. Sher G, Fisch JD. Vaginal sildenifil (Viagra): a preliminary report of a novel method to improve uterine artery blood flow and endometrial development in patients undergoing IVF. Hum Reprod 2000;15:806-9.
59. Stener-Victorin E, Waldenstrom U, Andersson SA, Wikland M. Reduction of blood flow impedance in the uterine arteries of infertile women with electro-acupuncture. Hum Reprod Biol 1996;11:1314-7.
60. Schenker JG, Meirow D, Schenker E. Stress and human reproduction. Eur J Obstet Gynecol Reprod Biol 1992;45:1-8.
61. Eugster A, Vingerhoets AJ. Psychological aspects of in vitro fertilization: a review. Soc Sci Med 1999;48:575-89.
62. Domar AD, Broome A, Zuttermeister PC, Seibel M. Friedman R. The prevalence and predictability of depression in infertile women. Fertil Steril 1992;58:1158-63.
63. Domar AD, Zuttermeister PC, Friedman R. The psychological impact of infertility: a comparison with patients with other medical conditions. J Psychosom Obstet Gynaecol 1993;14:45-52.
64. Mahlstedt PP, Macduff S, Bernstein J. Emotional factors in in vitro fertilization and embryo transfer process. J In Vitro fert Embryo Transf 1987;4:232-5.
65. Seibel MM, Taymore ML. Emotional aspects of infertility. Fertil Steril 1982;37:137-45.
66. Domar AS, Seibel MM, Benson H. The mind/body program for infertility: a new behavioral treatment approach for women with infertility. Fertil Steril 1990;53:246-9.
67. Chen A. An introduction to sequential electric acupuncture (SEA) in the treatment of stress related physical and mental disorders. Acupunct Electrother Res 1992;17:273-83.
68. Dong JT. Research on the reduction of anxiety and depression with acupuncture. Am J Acupunct 1993;21:327-30.
69. Luo H, Meng F, Jia Y, Zhao X. Clinical research on the therapeutic effect of the electroacupuncture treatment in patients with depression. Psychiatry Clin Neurosci 1998;52:S338-40.
Influence of acupuncture on the pregnancy rate in patients who undergo assisted reproduction therapy














ACUPUNCTURE
Those who received acupuncture increased their chances of conceiving by 65 percent.
February 8, 2008
Vittorio Hernandez – AHN News Writer
London, England (AHN) – Seven scientific trials among 1,366 women of different ages who found it difficult to conceive showed that having acupuncture at the same time the embryo was placed inside the womb during an in vitro fertilization procedure more than doubles the chance of the woman becoming pregnant.
The study was made by researchers at the University of Maryland School of Medicine and the VU University Amsterdam. It compared results of women who underwent acupuncture, those who were given fake needle treatments and those who had no extra therapy.
Those who received acupuncture increased their chances of conceiving by 65 percent, the study said. The British Medical Journal published the result of the medical breakthrough Friday.
While the study did not clearly explain how acupuncture aids fertility, experts theorized it could possible be the relaxing effect of acupuncture on the IVF procedure, considered extremely stressful.
Compared with repeated fertility treatment cycles which costs $7,785 (4,000 pound) per cycle in Britain, the acupuncture therapy is easier on the pocket.
One percent of births in the U.K. or 11,000 babies out of 32,000 IVF procedures are born every year in the U.K. The findings will be particularly significant for many western nations grappling with dwindling populations.